Insight
AI-Inferred Risk Adjustment in LEAD: A Consequential Shift
CMS’ LEAD model signals a shift from HCC-based risk adjustment to AI-inferred scores, reshaping how patient risk is measured and paid.

Fraud, waste, and abuse in healthcare is not a new problem. But the scale, sophistication, and operational impact of today’s activity is changing the conversation.
In the past year alone, federal agencies have intensified enforcement activity, expanded program integrity tools, and increased scrutiny on provider organizations, suppliers, and billing patterns across Medicare and Medicaid. At the same time, healthcare organizations are navigating increasingly complex reimbursement models where inappropriate utilization does not just create compliance exposure. It can directly affect benchmarks, shared savings performance, actuarial assumptions, and the overall economics of value-based care.
Recent federal actions make one thing clear: fraud, waste, and abuse is no longer just a compliance issue. It is becoming a strategic and financial risk issue for healthcare organizations operating under risk-based arrangements.
During a recent Arcadia Policy Pulse webinar, we explored how federal enforcement priorities are evolving, the types of fraud schemes emerging across the market, and what healthcare organizations can do to better identify and respond to suspicious utilization patterns.
Here are five key takeaways from the discussion.
Healthcare fraud enforcement activity has accelerated significantly over the past two years, particularly across Medicare, Medicaid, hospice, telehealth, durable medical equipment (DME), and high-cost specialty services.
For healthcare organizations participating in accountable care organizations (ACOs), Medicare Shared Savings Program arrangements, or other value-based care models, these trends have implications that extend well beyond compliance.
Improper utilization can distort:
This distortion is just one reason fraud, waste, and abuse in healthcare is increasingly becoming a strategic operational concern.
The Department of Justice and CMS are pursuing healthcare fraud cases more aggressively than at any point in recent memory.
In 2025 alone, the Department of Justice charged 324 defendants across all 50 states involving approximately $14.6 billion in alleged criminal fraud. Federal authorities also recovered $5.7 billion through False Claims Act cases tied to healthcare, alongside nearly 1,300 whistleblower actions.
The trend has continued into 2026.
Recent enforcement activity has included:
CMS is also expanding its program integrity toolkit. Recent actions include:
Collectively, these actions signal a more interventionist approach to healthcare program integrity.
Healthcare fraud schemes are becoming more sophisticated and harder to identify through traditional auditing methods alone.
Historically, healthcare fraud often involved clearly fraudulent activity, such as billing for nonexistent patients or submitting claims for services never delivered.

One of the biggest challenges for healthcare organizations is that modern fraud schemes often blend into legitimate clinical workflows.
Historically, healthcare fraud was easier to identify because it involved obviously inappropriate activity, such as billing for nonexistent patients or services never delivered.
Today's fraud schemes are more sophisticated.
Many involve:
The challenge is that these schemes often exploit gray areas between fraud, waste, and abuse.
For example, some high-cost skin substitute products entered the market with aggressive marketing campaigns and financial incentives that encouraged broader utilization. In some cases, clinicians may have believed they were providing appropriate care. In others, bad actors allegedly exploited reimbursement structures by applying excessive amounts of product or targeting vulnerable populations.
This is where healthcare organizations must think differently about surveillance.
The question is no longer simply whether a claim is valid. Organizations increasingly need to identify unusual utilization patterns, abrupt changes in coding behavior, geographic anomalies, and provider outliers that may indicate broader issues.
Healthcare claims analytics and benchmarking are becoming increasingly important for identifying emerging fraud, waste, and abuse patterns.
One of the most important lessons from recent fraud investigations is that many organizations cannot identify emerging patterns by looking at their own data alone.
Fraud schemes often appear statistically normal within a single organization or local market.
However, when claims data is analyzed across broader populations, unusual patterns become easier to identify.
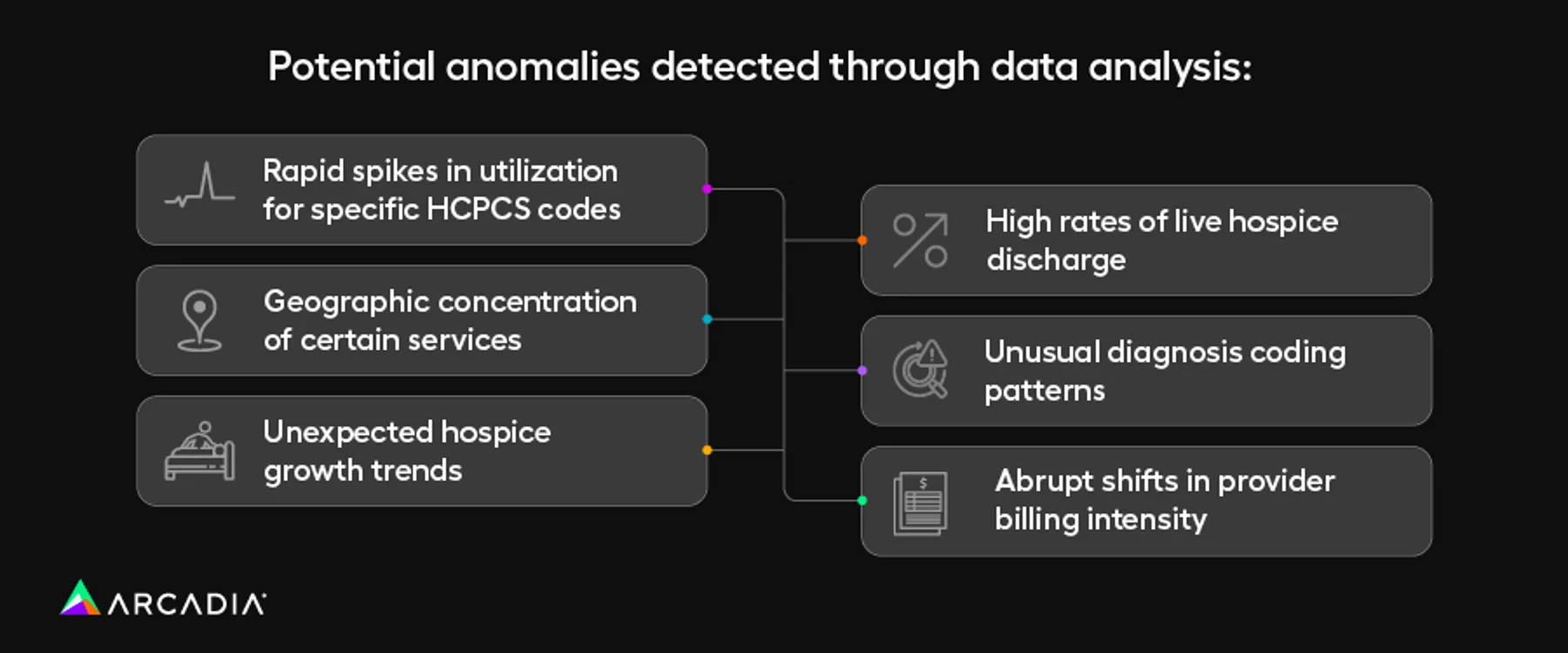
Examples include:
During our analysis, we found that benchmarking across organizations and regions can reveal signals that might otherwise remain invisible.
This is particularly important for accountable care organizations and other entities operating under value-based contracts, where inappropriate utilization can directly affect financial performance.
As healthcare fraud becomes more industrialized and data-driven, benchmarking and interoperability are becoming essential capabilities for effective oversight.
CMS is introducing new program integrity and utilization oversight mechanisms across traditional Medicare and Medicaid.
For years, traditional Medicare has operated with fewer prospective utilization controls than commercial insurance or Medicare Advantage.
That may be changing.
CMS is increasingly experimenting with prospective oversight models aimed at preventing inappropriate utilization before payment occurs. One example is the WISER model, which introduces prior authorization-like reviews for selected services in traditional Medicare.
The rollout has generated debate.
On one hand, many stakeholders acknowledge the need for stronger controls in areas vulnerable to inappropriate utilization. On the other hand, early implementation challenges have raised concerns about delays in care and administrative burden.
This reflects a broader tension across healthcare policy.
Healthcare organizations need mechanisms that reduce inappropriate utilization and fraud. But they also need systems that preserve patient access and avoid creating new barriers to medically necessary care.
The long-term challenge will be balancing program integrity with operational fairness and clinical appropriateness.
Healthcare organizations participating in value-based care need more proactive approaches to fraud, waste, and abuse monitoring.
One of the clearest themes from the discussion was that healthcare organizations increasingly need to view fraud, waste, and abuse detection as part of broader operational stewardship.
Organizations operating under risk-based arrangements are financially exposed to inappropriate utilization, even when they are not directly responsible for the underlying activity.
That means provider organizations, ACOs, health systems, and payers all have a stake in:
In many cases, the most effective defense is not a dedicated fraud program. It is a culture of clinical appropriateness combined with strong medical economics monitoring.
Organizations that already focus on efficient, evidence-based care delivery are often better positioned to identify suspicious utilization patterns before they become widespread problems.
Fraud, waste, and abuse will remain a major focus for federal regulators in the years ahead. At the same time, healthcare organizations operate in an environment of increasing financial pressure, growing administrative complexity, and rapidly evolving technological capabilities.
Those dynamics create both risk and opportunity.
Artificial intelligence and advanced analytics may help organizations identify suspicious patterns faster and more accurately than ever before. But the same technologies may also enable more sophisticated fraud schemes.
The organizations best positioned for the future will be those that combine strong data visibility, operational discipline, and clinical oversight with the ability to adapt quickly as the regulatory landscape evolves.
Fraud, waste, and abuse is no longer a peripheral compliance concern. It is becoming a core operational challenge for modern healthcare organizations.
Fraud involves intentional deception for financial gain. Waste refers to unnecessary or low-value healthcare spending that may occur without malicious intent. Abuse typically involves practices that exploit payment structures or reimbursement incentives in ways that increase inappropriate utilization.
Organizations participating in value-based care arrangements are financially exposed to inappropriate utilization trends. Fraudulent or excessive spending can affect benchmarks, shared savings calculations, utilization trends, and population health performance.
Healthcare organizations can use claims analytics, benchmarking, utilization monitoring, provider outlier analysis, and interoperability tools to identify unusual utilization spikes, coding changes, or geographic anomalies.
CMS is expanding prospective oversight through initiatives such as the WISER model, provider enrollment scrutiny, Medicaid provider revalidation, and increased monitoring of significant and anomalous billing trends.