Technology infrastructure improves success
To succeed in CMS’ ASM model, provider organizations will require robust data infrastructure and advanced analytics tools that align with the model’s requirements. Three technology-enabled capabilities are especially critical:
1. Performance Intelligence for Transparency and Benchmarking
Success in ASM hinges on transparency and the ability to benchmark performance across large populations and peer groups. Look for solutions that offer:
- Access to nationwide and market-level analytics that encompass hundreds of millions of beneficiaries and millions of providers.
- Risk-adjusted scoring methodologies that enable reliable comparisons across provider performance.
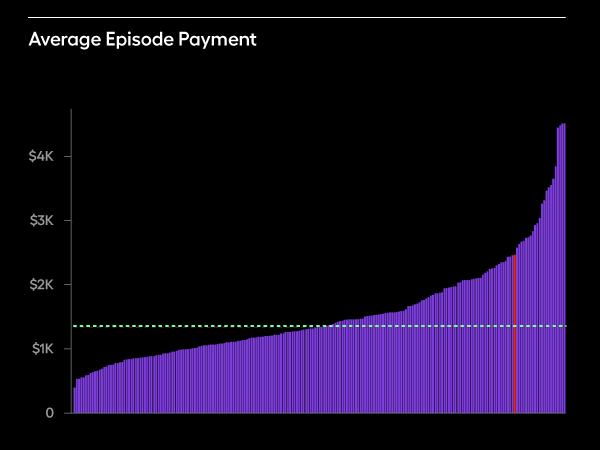
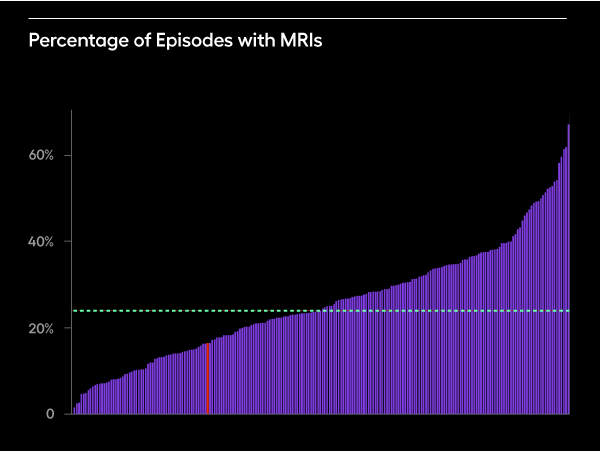
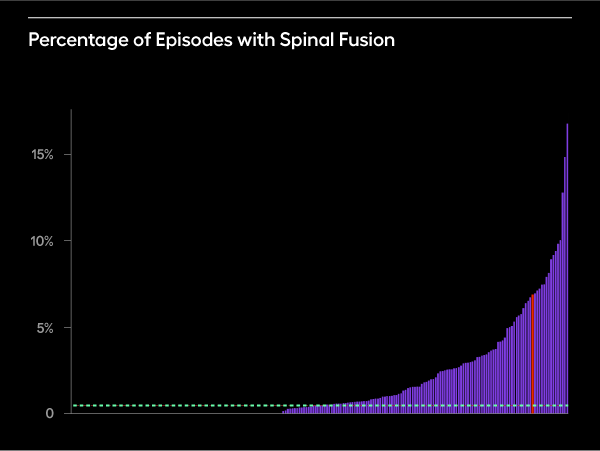
- Episode-based cost measurement frameworks that align directly with conditions prioritized under ASM, such as heart failure and low back pain.
These capabilities allow organizations to understand relative performance, surface variation, and drive targeted improvements—all foundational to ASM’s transparency and accountability goals.
2. Point-of-Care Insights to Drive Quality Measurement
ASM places a strong emphasis on chronic disease management and quality measurement. Tools that surface longitudinal patient data within clinical workflows—without disrupting provider efficiency—are essential. Capabilities that participating organizations need include:
- EHR-integrated decision support for timely access to comprehensive patient histories.
- Intelligent risk stratification to proactively manage high-risk populations.
- Automated quality gap closure workflows that align with ASM’s reporting and incentive structure.
These insights empower providers to make informed decisions in real-time, which is critical for improving outcomes under ASM’s quality-focused framework.
3. Technology-Enabled Care Coordination for Targeted Conditions
Effective care coordination is required under ASM, especially for high-cost, high-need patients with heart failure or low back pain. Look for technology that can:
- Predictively identify high-risk individuals using condition-specific models.
- Automate workflow routing to streamline care team operations and reduce administrative burden.
- Embed evidence-based guidelines into care planning, supporting consistent, high-quality interventions.
Arcadia's comprehensive healthcare data platform aggregates clinical, claims, social determinants, and pharmacy data in real-time. Our platform's proven value-based care success—including 41.5% ED visit reductions for COPD patients and enabling care teams to serve 3x more patients—demonstrates the capabilities needed to drive ASM-required outcomes.