An ACO assignment journey: Coding and attribution in medicare ACOs
By
Daniel Eklund, Contributing Author at Algorex Health, Luke Shulman, Contributing Author at Algorex Health, and Nick Stepro, Chief Technology Officer and President of Tech and Data at Arcadia
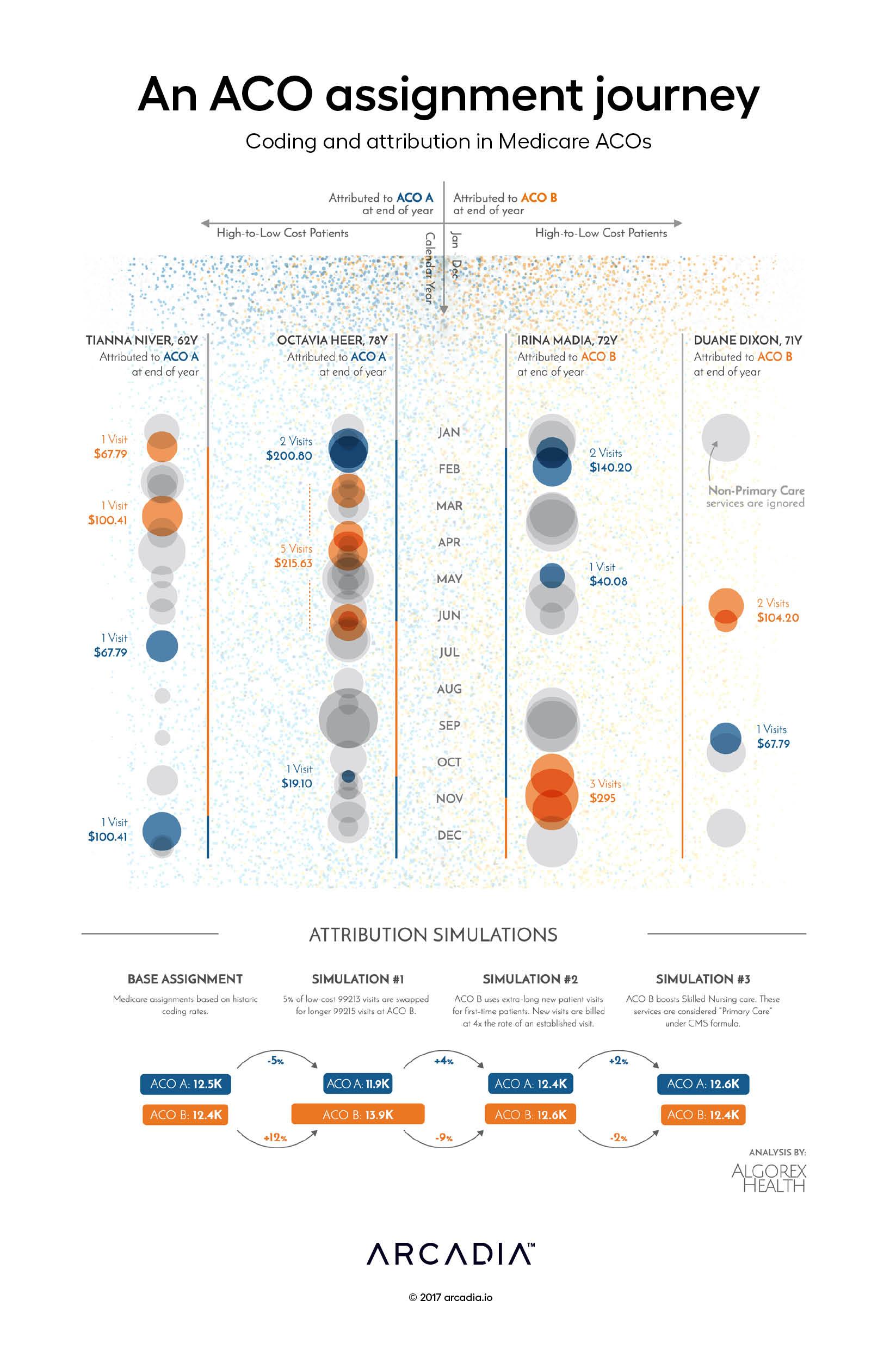
In this figure, the artists re-imagine the process by which individuals are assigned to an ACO as a battleground, on which ACOs competing for clientele and risk hope to effectively balance their patient load to optimize the utilization of available resources and maximize the creation of shared savings.
Here, four Medicare beneficiaries are tracked throughout the calendar year. With the behavior (and physician choices) of the beneficiaries fixed — they are unconstrained in the ACO marketplace so this assumption is not too removed from reality — we are forced to consider how the operational choices of the ACO influence the assignment process.
As presented, two of the beneficiaries are assigned to ACO A, while the other two beneficiaries are assigned to ACO B. At the end of the year, this assignment of responsibility will be applied to the ACO, irrespective of their engagement strategy.
However, if we consider the assignment process a strategic effort — a game of optimization — we can explore several opening moves:
First move: ACO B starts an initiative to expand visits by existing patients with certain high-risk conditions, replacing certain moderate acuity visits with detailed evaluations. This results in increased assignments to ACO B, as tie-breaking assignments (like Tianna Niver) side with the costlier provider.
Second move: ACO B expands their new patient visits substantially, billing for those patients at a vastly higher rate. However, this expansion in time results in a drop-in ability to schedule new patients (like Duane Dixon), resulting in lower than expected expansion and a decline in newly assigned members.
Third move: ACO B expands the use of skilled nursing primary care billing. This allows ACO B to count nursing care toward assignments for higher acuity patients (like Octavia Heer), but also replaces some costlier encounters with less expensive nursing encounters, resulting in little net change in assignments.
This battle for assignments continues into the next year, and as the ACOs gather more and better information about their patients, both assigned and unassigned, they continue to strive for the best alignment of their care capabilities, their patients, and their success strategy.
Prepared in collaboration with Algorex Health, helping ACOs use data beyond claims to understand patient engagement.
The American College of Surgeons (ACS) and Arcadia announced a new collaboration to support the ACS Clinical Data Strategy, modernizing how surgical clinical data is collected,...
The CY2027 Physician Fee Schedule signals a real shift toward value-based care: new ACO growth incentives, higher reimbursement for MSSP and LEAD participants, looser beneficiary...
Healthcare analytics software transforms raw data into actionable insights. Explore these top providers to choose the best solution for your healthcare team.