Insight
AI-Inferred Risk Adjustment in LEAD: A Consequential Shift
CMS’ LEAD model signals a shift from HCC-based risk adjustment to AI-inferred scores, reshaping how patient risk is measured and paid.

Editor’s note: This is the fourth article in a series about CMS’ new LEAD model. Article one explored the new model in broad strokes. Article two discussed AI-Inferred Risk Adjustment. Article three explored benchmarking. Future posts will explore beneficiary enhancements.
Accountable care organizations have always had a challenge integrating specialists into value-based care programs. LEAD’s (Long-term Enhanced ACO Design) new CMS-Administered Risk Arrangements (CARA) initiative is CMS’ attempt to solve the operational part of that problem. ACOs were designed around the idea that total cost of care accountability for a set of patients leads to more thoughtful resource stewardship. At the heart of successful ACOs are well-run primary care practices who prevent downstream expensive treatments such as hospitalizations, emergency department visits, and avoidable procedures, thereby reducing the total cost of care and improving outcomes. This premise has driven real savings in both MSSP and ACO REACH.
Unfortunately, most Medicare spending is not on primary care. It’s the cardiologist who decides how often a patient with heart failure receives cardiac imaging. It’s the orthopedist who determines whether a knee replacement happens now or after six months of conservative management. It’s the rheumatologist choosing among treatment protocols that may differ by tens of thousands of dollars and produce similar outcomes. Often specialty input is appropriate, but the accountability surfaced to primary care physicians in the ACO model hasn’t percolated to specialty consultants.
ACOs have historically struggled to meaningfully incorporate specialists into their value-based programs. The challenge is that the incentive structure for specialists and ACOs typically point in different directions. An ACO wants to reduce unnecessary utilization. While both primary care and specialty physicians are paid for volume even in an ACO model, primary care access and volume are fundamentally more oriented to preventive care than specialty services. The specialist toolkit is more likely to include high-cost imaging, Part B therapies, and procedural care. Furthermore, joining an ACO adds administrative burden, imposes a layer of oversight, and offers uncertain financial benefits in return. Finally, there’s the reality that because specialty compensation can be several times that of primary care compensation, a $1 shared savings incentive has less value to a specialist than to their primary care colleague. The result is that most ACOs function as primary care risk arrangements with a specialist challenge that they manage indirectly, through referral patterns and care protocols, rather than through shared financial accountability.
LEAD’s new CARA initiative is CMS’ attempt to make specialist value-based arrangements operationally feasible for ACOs.
CARA is an infrastructure play. CMS is offering to administer episode-based risk arrangements on behalf of ACOs. Administer is the key word. In practice, that means the ACO and a specialist can agree to share upside, downside, or both kinds of risk for a defined episode of care, with CMS handling the underlying mechanics. In prior attempts to bring specialists into value-based arrangements, the burden fell on the ACO who needed to identify the right specialists, negotiate contracts with episode definitions and target prices, build the data infrastructure to track episode performance, calculate who owed what at the end, and handle the payment flows. For most ACOs, this was either prohibitively complex or prohibitively expensive, and frequently both. The result was that specialist engagement happened in theory and not as much in practice.
Under CARA, CMS becomes the administrator. The ACO and a specialist group agree on the terms of an arrangement. CMS handles episode tracking, performance calculation, and payment flows. The ACO doesn’t need to build the infrastructure. The specialist group may not need to work from a one-off ACO-specific framework, because CMS is providing a common episode and contracting infrastructure. The plumbing is standardized. The ACO and specialist just have to agree to use it.
The idea of bringing specialists into value-based care is not new. What is new is CMS trying to reduce the operational friction that’s kept that idea from becoming routine practice. LEAD’s CARA approach is novel in that it lowers the operational barrier to achieving accountability in practice. Whether the barrier is actually low enough to produce widespread specialist engagement is the real question, and we won’t know the answer until participating ACOs start working through the details. But the intent is clear. We see a strong focus from CMS on integrating specialty care into value-based care through mandatory models such as TEAM, Ambulatory Specialty Model, and the newly proposed CJR-X. CARA provides ACOs and specialists with a voluntary opportunity to bring value to specialty care on their own terms.
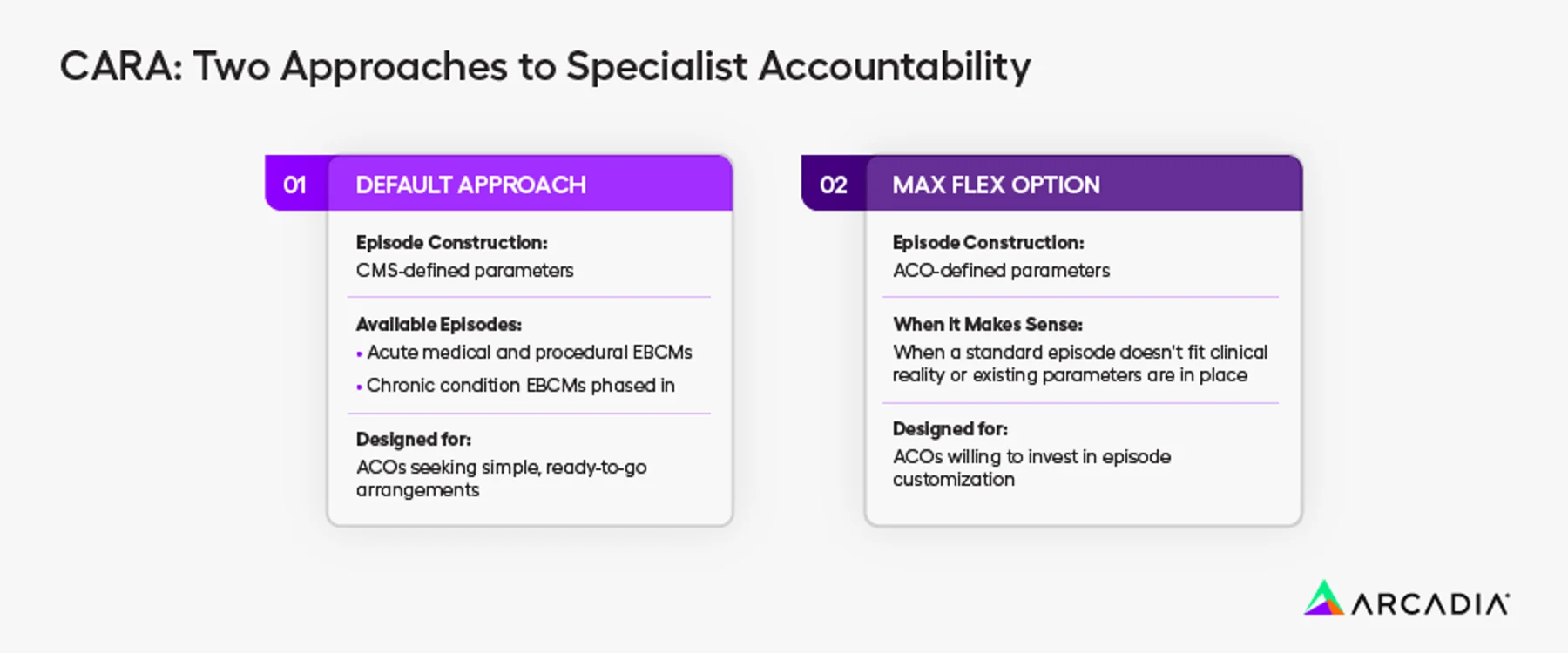
CARA offers two flavors of specialist accountability. An ACO that wants standardized infrastructure with minimal design work can use the Default Approach. An ACO with sophisticated analytics capabilities and a specialist partner willing to invest in episode customization can go further with Max Flex. The program is designed to be usable across a range of organizational sophistication levels.
The Default Approach uses CMS-defined episode parameters: standardized definitions of what triggers an episode, what services are included, how long the episode runs, and the methodology for calculating performance. CMS says CARA will launch with acute medical and procedural Episode-Based Cost Measures (EBCMs) and phase in chronic condition EBCMs early in the initiative. The Default Approach is designed for ACOs that want to get into specialist arrangements without the complexity of building custom episode logic from scratch.
The Max Flex Option allows the ACO and the specialist to customize the episode construction: the trigger codes, the episode length, what is included or excluded. This is for situations where the standardized episode does not fit the clinical reality, or where an ACO and a specialist group have already agreed on specific parameters that make more sense for their relationship and patient population.
Both approaches use EBCM methodology, and performance is calculated against episode-specific target prices that the ACO and the Preferred Provider negotiate. CMS supplies the episode infrastructure and makes payments to ACOs and Preferred Providers based on the episode-based risk arrangements they establish.
The most specific episode in CARA at launch is called RISE to Age in Place—Resilience and Independence in a Safe Environment. It’s a falls prevention episode that’s worth understanding because it illustrates how CMS thinks about the scope of what an episode can include. This is an evolutionary leap from familiar procedure bundles.
Falls are a major driver of Medicare spending, not just in the cost of treating injury but also in the risk that falls and injury pose to independent living. A serious fall in an older adult can mean an emergency department visit, an inpatient stay, a rehabilitation admission, and a cascade of downstream care needs which are expensive and potentially avoidable. The standard healthcare response to fall risk is clinical: physical therapy, medication review, and balance assessment. These are valuable, but not enough.
The RISE episode includes conventional coordinated care delivery by occupational therapists and registered nurses. What’s less conventional is that it also allows for payment for structural home modifications—things like grab bars, ramp modifications, and better lighting—up to $2,500, where specified in the episode terms. This is CMS acknowledging, in a payment model, that the home environment is part of the clinical problem. The risk factors for a serious fall are partly clinical and partly physical. Addressing the physical factors requires interventions that traditional Medicare doesn’t cover and that traditional episode-based models haven’t included.
This isn’t a policy statement about social determinants of health. It’s a practical program design choice: if you’re going to reduce falls and the costs they generate, you must address the reasons falls happen. RISE is an attempt to build an episode that actually covers the range of interventions needed. It also illustrates a challenge in episode-based models that align with prevention: the one-year time horizon may not be sufficient to capture the savings associated with an avoided event.

CMS is initially testing CARA within LEAD among Global Risk ACOs. Professional Risk ACOs (those bearing 50% shared savings and losses rather than 100%) cannot participate at the outset, although CMS opens the door for that possibility later in the model. This is a coherent design choice, not an arbitrary restriction. An ACO bearing full two-sided risk on its total cost of care has a direct financial incentive to reduce specialist-driven costs. An ACO bearing half the risk has a weaker and more complicated incentive. Episode-based arrangements with specialists make the most sense when the ACO has a clear economic interest in the episode’s outcome. Global Risk creates that interest more intensely than Professional Risk.
Importantly, CARA is voluntary. Global Risk ACOs aren’t required to establish episode arrangements with any specialist group. An ACO can participate in LEAD at the Global Risk level, take full advantage of the capitation tools and benchmark structure, and never participate in CARA at all. This means CARA’s adoption will depend on whether ACOs and their specialist partners find value that exceeds the administrative efforts.
CARA makes more sense when viewed alongside TEAM. TEAM creates mandatory episode-based accountability for a defined set of hospital-based procedures. CARA is the ACO-side complement: a voluntary mechanism that lets ACOs and specialists create episode-based accountability within a broader total-cost-of-care model.
Without something like CARA, LEAD and TEAM risk operating as parallel structures. TEAM can hold hospitals accountable for selected episodes; CARA gives ACOs a way to build financial alignment with specialists around those episodes and others beyond TEAM’s scope. If it works, it could connect hospital episode accountability to the ACO’s broader cost and care-management strategy.
The LEAD Request For Applications (RFA) describes CARA’s structure and principles, but several critical details are still outstanding. CMS has published a broad set of EBCMs under consideration, but some operational details about how the full menu will be implemented remain outstanding. CMS hasn’t yet specified parameters for chronic condition episodes, such as which conditions, what triggers, and what episode lengths. CMS described the negotiation process for Max Flex episode construction at a high level, but not in the operational detail that a participating ACO would need.
There is also a practical question that no documentation answers yet: what does the CARA participation process actually look like for a specialist group? The ACO’s perspective—sign the LEAD Participation Agreement, execute a CARA Amendment, and designate Preferred Providers—is reasonably clear from the RFA. The specialist’s perspective—what they are agreeing to, what financial exposure they are taking on, what data they will receive, and how disputes are resolved—is less detailed. Specialists who might be interested in becoming Preferred Providers will need concrete answers to these questions before they can seriously evaluate participation.
If CARA works, it could give ACOs a standardized way to turn specialist alignment from a talking point into an actual financial arrangement.
Erica Everhart leads policy and payment model strategy at Arcadia. She writes about the intersection of CMS policy, healthcare analytics, and the practical realities of value-based care. Data referenced in this article is from the LEAD Request for Applications released March 31, 2026.